We use cookies on this site to enhance your experience.
By selecting “Accept” and continuing to use this website, you consent to the use of cookies.
Feb. 10, 2015
By: Jeff Grischow
In April 2015 Niger’s Health Minister Mano Aghali reported a serious outbreak of meningitis, with 1,150 cases and 85 confirmed deaths. The announcement came on the heels of the World Health Organization’s recent approval of a new and cost-effective vaccine. The vaccine emerged out of the ten-year program – the Meningitis Vaccine Project (MVP) – launched in 2001 with support from the Bill and Melinda Gates Foundation. Structured as a partnership between the WHO, the health organization PATH, and the Serum Institute of India, the MVP developed the vaccine successfully by 2010. Between 2010 and 2015, the MVP carried out an initial mass vaccination campaign targeting 215 million people in 15 African countries. Its success led the WHO to approve the vaccine for general use in January 2015.
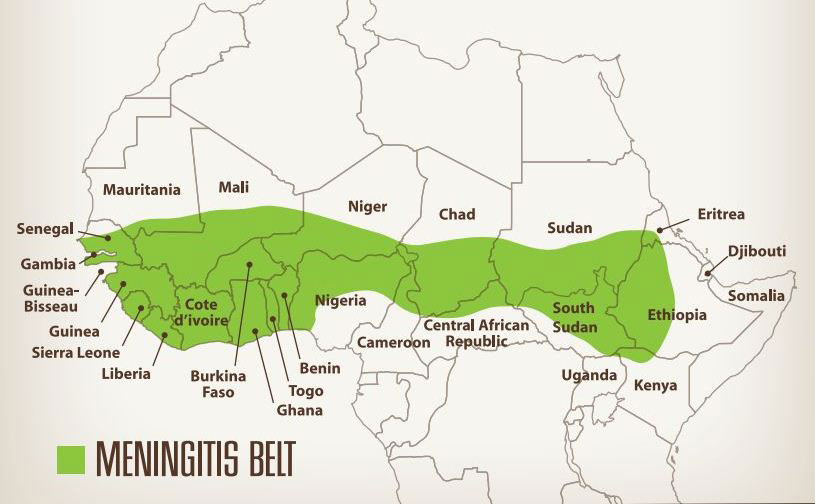
Meningitis is a relatively recent global disease. It first appeared in Geneva in 1805 and New England in 1806 (Greenwood, 1999, 341). The first recorded outbreak in Africa occurred among French soldiers in Algiers in 1840, and by the 1880s it had spread to southern Africa (Greenwood, 1999, 341-3; Greenwood, 2006, 773). The first known outbreak in West Africa occurred in northern Nigeria in 1906, possibly carried back by West Africans who had travelled to present-day Sudan on their way to Mecca or supporting the anti-colonial uprising of the Mahdi. The Nigerian epidemic soon spread to northern Ghana and it affected tens of thousands of people. By this time, the scientific community had discovered the parasite responsible for the disease, but an effective vaccine eluded medical researchers for almost one hundred years. As a result, meningitis continued to plague communities across Africa’s ‘meningitis belt’ stretching from Senegal to Ethiopia. In fact, the biggest epidemic in Africa’s history broke out very recently, in 1996-7, claiming 25,000 victims. It was this event that prompted a number of African governments to approach the World Health Organization to find a solution, resulting in the MVP.
The present outbreak carries two lessons. First, there must be better international mechanisms for delivering the new vaccine to the affected countries. Niger, for instance, only possesses about half of the 1.2 million doses it needs. More fundamentally, the events in Niger illustrate that we know little more than we did a hundred years ago about why outbreaks appear ‘in a particular place at a particular time’ (Greenwood, 2006: 777-8). For this reason, perhaps we should take to heart Greenwood’s call for more research into the ‘carriage of the group A meningococcus in the African meningitis belt and the factors that influence it, for example the effects of age and season and the impact of the host’s immune response’ (Greenwood 2006, 779). In Greenwood’s opinion, the key area for future research must be the ‘epidemiology of nasopharyngeal infection with the meningococcus in Africa’ (Greenwood 2006, 779). Without this research, it may prove very difficult to predict the most important locations for mass immunization before tragic outbreaks like to one in Niger occur.
Image source: Africa’s Meningitis Belt, 2009 (http://www.humanosphere.org).